PCOS is an endocrine and metabolic disorder. It is considered in any woman with acne, hirsutism, menstrual irregularity, or obesity.
Patients with PCOS, have anovulation, i.e. they may not produce a follicle cyclically. They may therefore present with primary amenorrhea (i.e. no periods at all), too few periods (oligomenorrhea) or secondary amenorrhea i.e. absence of periods for six months or more. Some may also have excessive, frequent and irregular bleeding (dysfunctional uterine bleeding).
Resistance to insulin, and increase in insulin levels is an important factor in PCOS. Obesity is present in approximately one-half of patients with PCOS. The waist:hip ratio may be greater than 0.85.
The cause of PCOS is unknown, but there is a possibility that PCOS may be a complex genetic disorder in which the genetic factor interacts with various environmental factors and causes imbalance in the hormones.
The diagnosis of PCOS is based upon clinical and biochemical criteria. It is suspected in cases of adolescents with hirsutism, acne, menstrual irregularity, or obesity. The diagnosis is further confirmed if excess androgen is demonstrated by laboratory testing. Androgen panel consists of plasma total testosterone, free testosterone, and another androgens such as DHEA sulfate. Plasma-free testosterone is the single most sensitive test for the detection of androgen excess. DHEA sulfate is the main marker of androgens that come from adrenals. Cortisol and thyroid function tests are indicated in obese patients to exclude other causes of obesity.
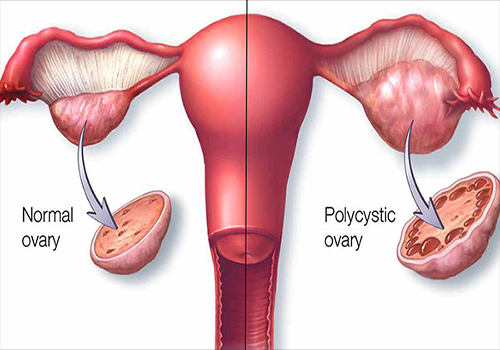
Pelvic ultrasound shows the features of a polycystic ovary. i.e. multiple(more than 10) small follicles with increased stroma.
A baseline lipid panel and a glucose tolerance test are important as PCOS is related to insulin resistance. The fasting glucose concentration is poor predictor of the two-hour level in PCOS. Two-hour blood glucose greater than 140 mg/dL indicates insulin resistance and this is important from the treatment point of view.
Treatment:
The treatment of PCOS is based upon the symptoms. The choice of treatment will depend on the individual patient’s symptoms and goals.
Reduction in weight by diet and exercise is essential first step.
Menstrual irregularity should be treated in patients with PCOS because chronic anovulation is associated with increased risk of developing endometrial hyperplasia and carcinoma.
Combined Oral contraceptive pills (COCP) therapy usually is the first-line treatment for women with menstrual irregularity. They regularize the cycles very effectively and also normalize androgen levels.
Cosmetic treatment of abnormal and excessive hair growth is offered to patients. It is safe and effective but does not correct the underlying problems. Therefore they all offer only temporary relief. The usual methods are depilation (e.g. shaving, hair removing creams), epilation (eg, plucking, waxing), destruction of the dermal papilla (eg, electrolysis or laser therapy.
Cosmetic treatment of abnormal and excessive hair growth is offered to patients. It is safe and effective but does not correct the underlying problems. Therefore they all offer only temporary relief. The usual methods are depilation (e.g. shaving, hair removing creams), epilation (eg, plucking, waxing), destruction of the dermal papilla (eg, electrolysis or laser therapy.
Treatment with COCP brings about significant improvement in acne and arrests progression of hirsutism.
Antiandrogens are sometimes prescribed in combination with COCP in severe hirsutism. Insulin-lowering agents such as metformin, thiazolidinediones and D-chiro-inositol are used to correct the insulin resistance. This improves ovulation and hormonal profile in patients with PCOS.
Antiandrogens are sometimes prescribed in combination with COCP in severe hirsutism. Insulin-lowering agents such as metformin, thiazolidinediones and D-chiro-inositol are used to correct the insulin resistance. This improves ovulation and hormonal profile in patients with PCOS.
Patients with PCOS who desire child bearing and do not conceive naturally may require ovulation drugs and assisted reproductive techniques to help them conceive.
Above all patients with PCOS require a boost to their confidence as they may have serious emotional issues with their hair growth, acne and obesity.